CCS: Clinical Consensus Selection for Radiology Report Generation
Why CCS? 🔬
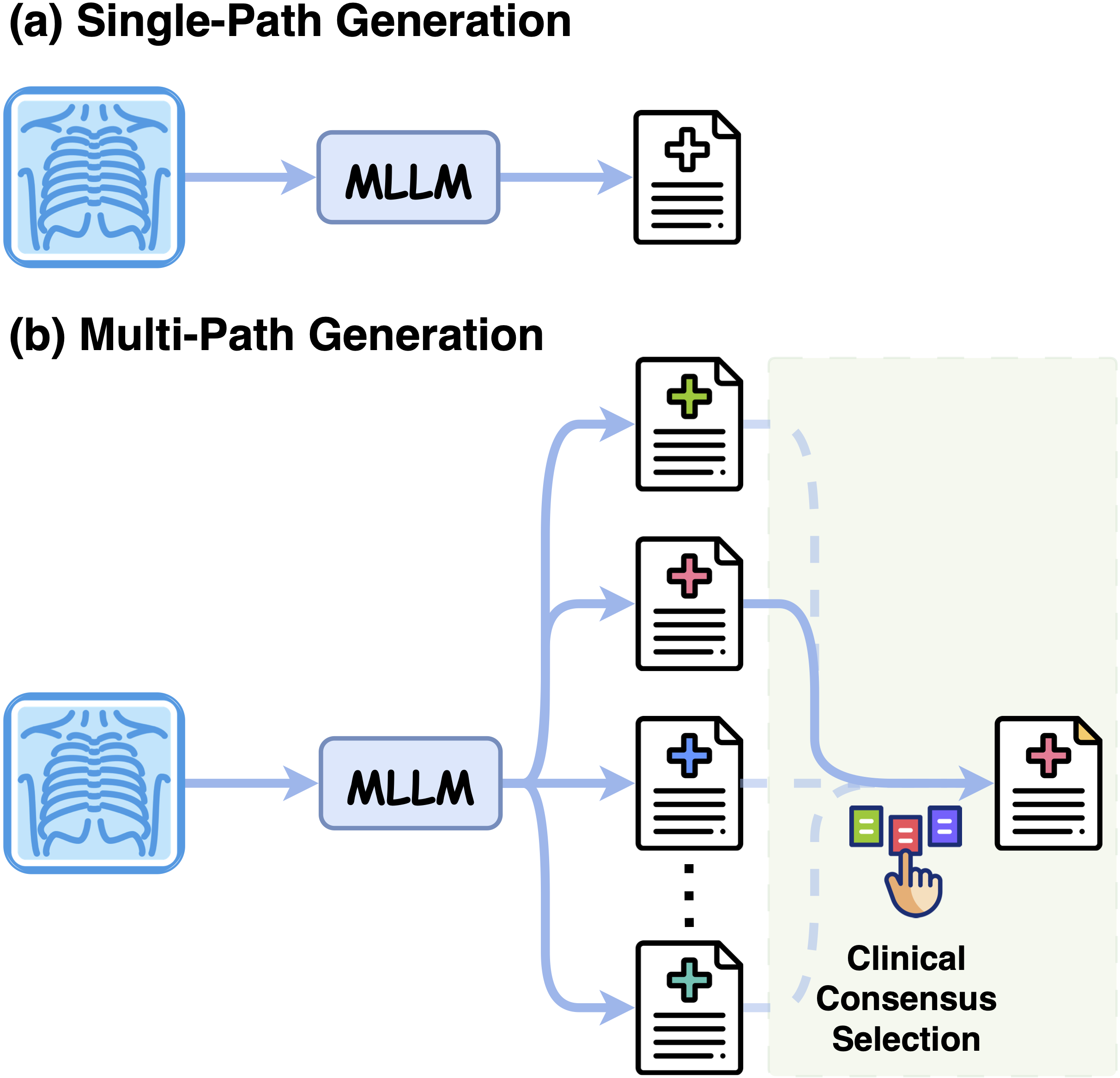
Most radiology MLLMs commit to a single decoded report token by token, so one unfavourable step can omit a finding or assert one unsupported by the image, with no way to recover. Yet a fixed model often places clinically stronger reports elsewhere in its candidate pool — the bottleneck is not what the model can generate, but which candidate it commits to.
How CCS Works ⚙️
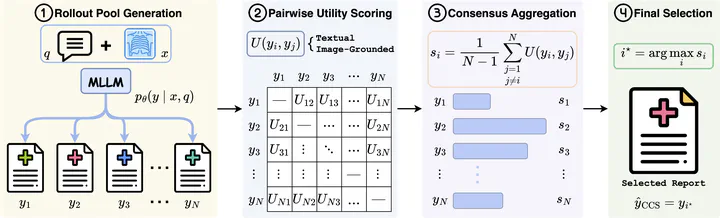
Clinical Consensus Selection (CCS) is a reference-free, decoder-agnostic inference-time framework that reframes RRG as candidate selection — no retraining or extra parameters.
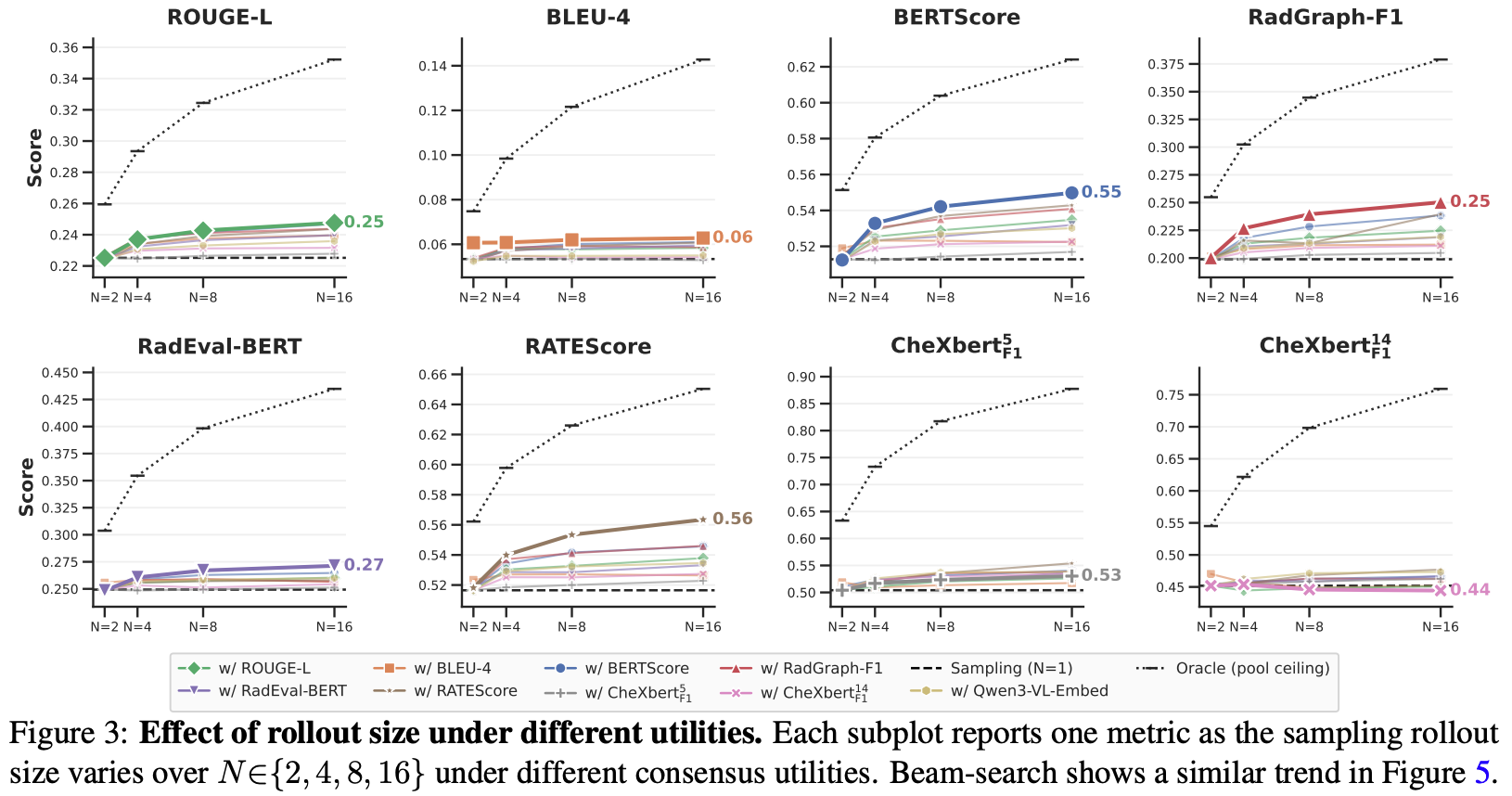
- Rollout sampling: draw N candidate reports from the radiology MLLM via stochastic decoding.
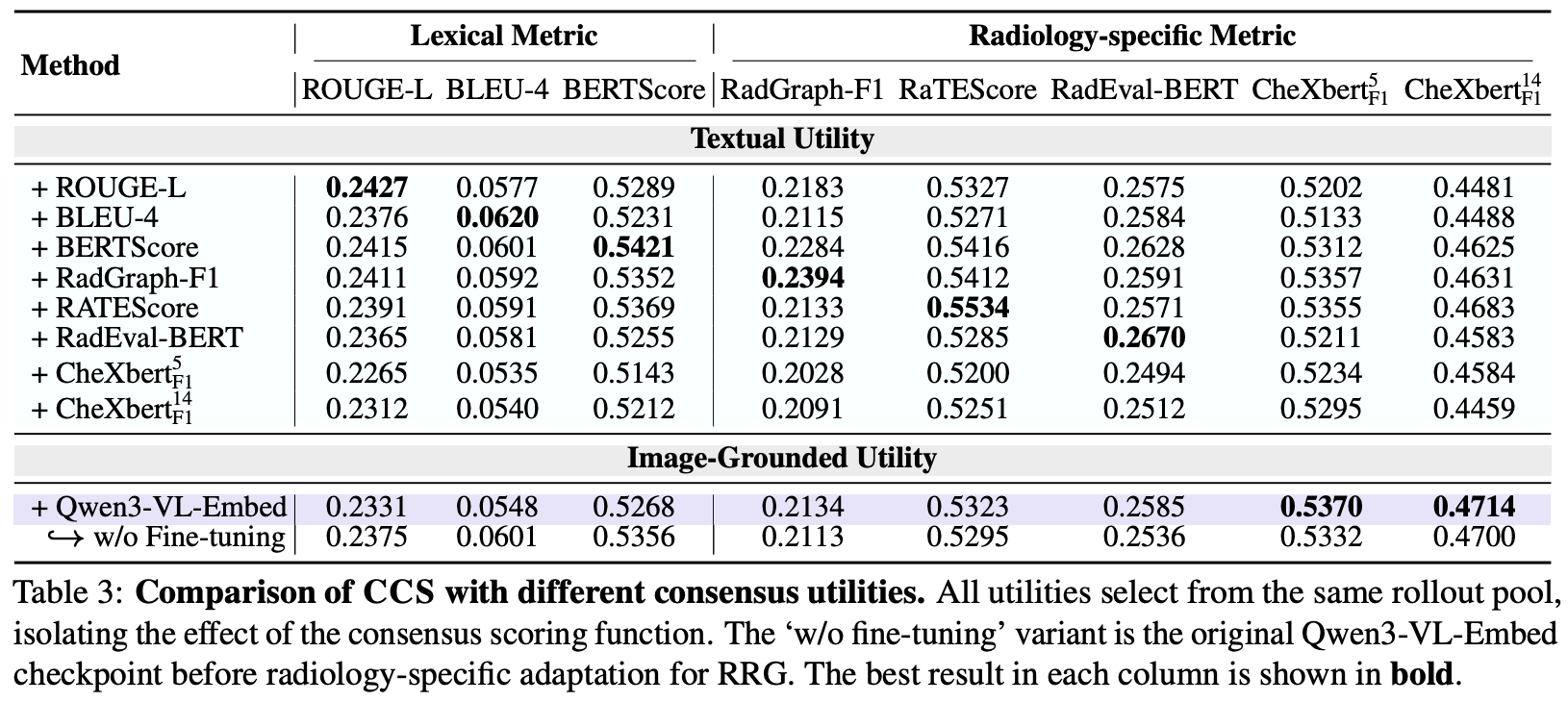
- Textual consensus utility: repurpose report-evaluation metrics as reference-free pairwise agreement scores.
- Image-grounded utility: measure candidate agreement with Qwen3-VL-Embed, a multimodal embedder adapted on image–report pairs, capturing clinical agreement beyond surface text.
- Highest-consensus selection: return the candidate with the highest mean pairwise consensus over the pool.
Key Contributions ✨
- Inference-time perspective: We show candidate pools routinely contain reports with higher clinical reliability and consistency than single-path outputs.
- CCS framework: A decoder-agnostic Best-of-N method that aggregates pairwise clinical consensus using both textual and image–report-adapted multimodal utilities.
- Consistent gains: Across three datasets and multiple radiology MLLMs, CCS improves RRG at inference time and identifies image-grounded utility as a distinct selection axis.
Main Results 📈
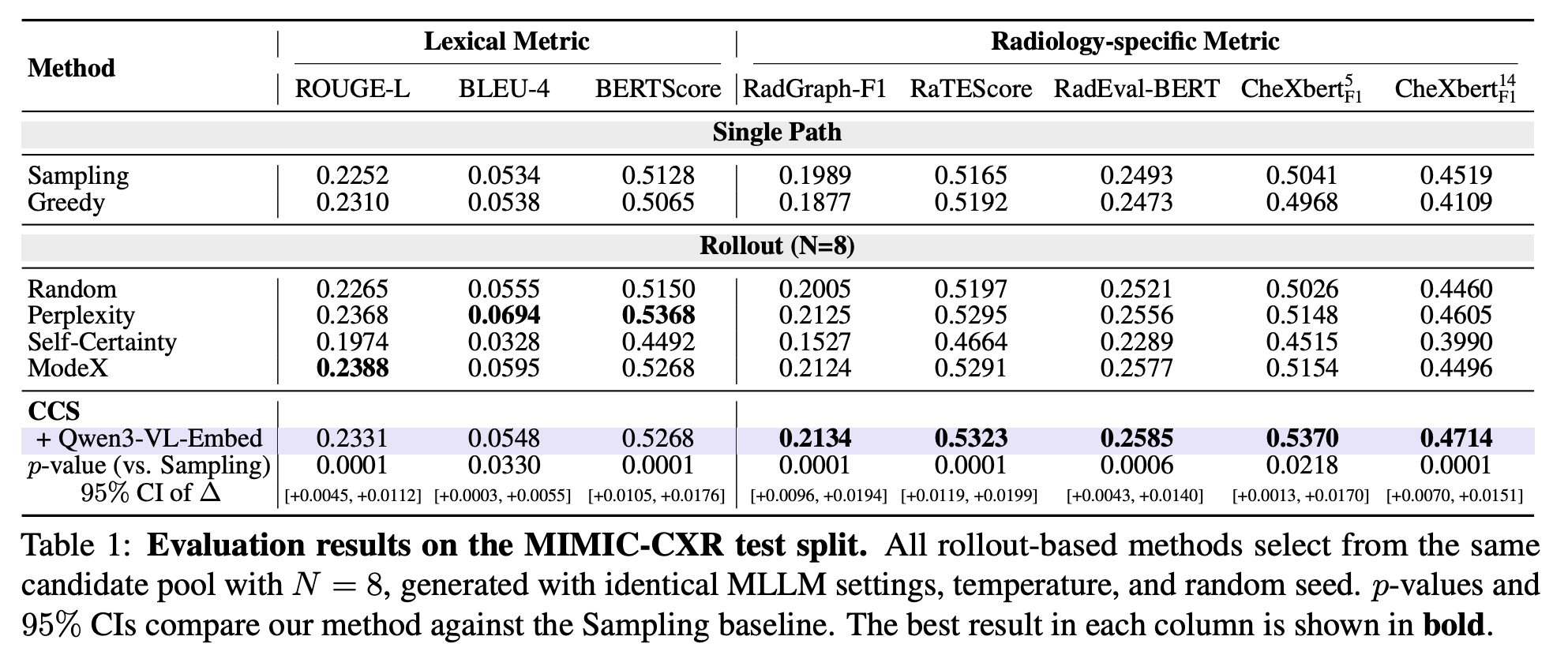
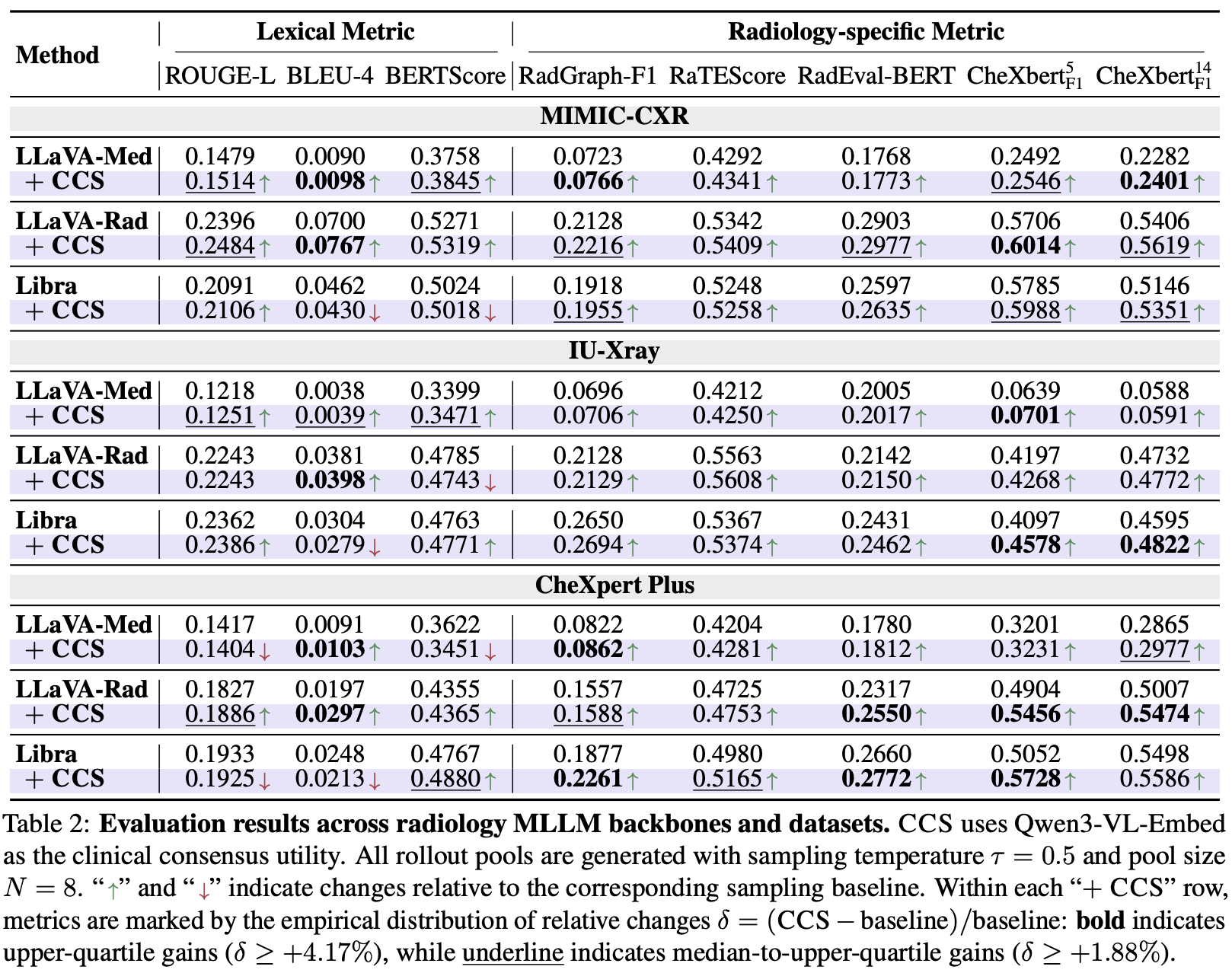
On MIMIC-CXR, CCS improves all radiology-specific metrics over Sampling (e.g. RadGraph-F1 0.1989 → 0.2134, CheXbert-F1⁵ 0.5041 → 0.5370), with gains statistically significant (p < 0.05). Unlike generic Best-of-N selectors (Self-Certainty, ModeX) that give inconsistent or negative clinical gains, CCS improves consistently across all backbones and datasets.
Analysis 📊
Per-label F1 shows CCS recovers abnormal findings that text-only consensus suppresses — confirming that image-grounded utility is a selection axis distinct from textual consensus, with substantial headroom still remaining.
Case Study 🔍
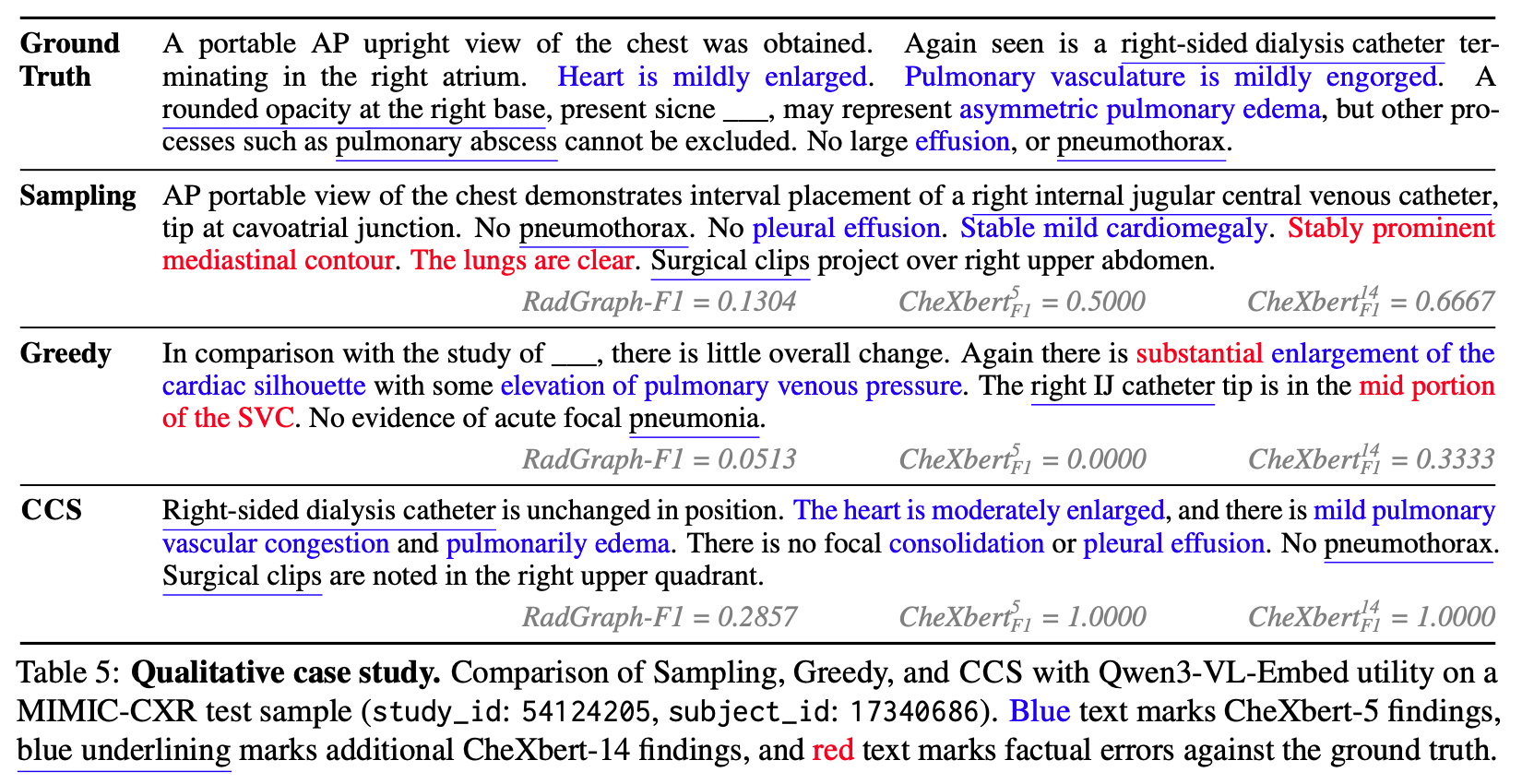
On a real MIMIC-CXR case, single-path decoding asserts factual errors (false “clear lungs”, mislocalised catheter), whereas CCS selects a more image-grounded report (CheXbert-F1⁵ 1.0000 vs Sampling 0.5000).
BibTeX 📚
@article{zhang2026ccsclinicalconsensusselection,
title={CCS: Clinical Consensus Selection for Radiology Report Generation},
author={Xi Zhang and Yingshu Li and Zaiqiao Meng and Jake Lever and Edmond S. L. Ho},
year={2026},
eprint={2605.30131},
archivePrefix={arXiv},
primaryClass={cs.CL},
url={https://arxiv.org/abs/2605.30131},
}